Gallstones are one of the risk factor for gallbladder cancer. Quite few patients with gallbladder cancer have gallstones at the time of diagnosis. Stone size of more than 3cm increases the risk of gall bladder cancer.

Gall Bladder & Bile Duct Cancers
Malignant Biliary Cancers
This includes gall bladder cancer and bile duct cancers (hilar cholangiocarcinoma).
Gall Bladder Cancer:
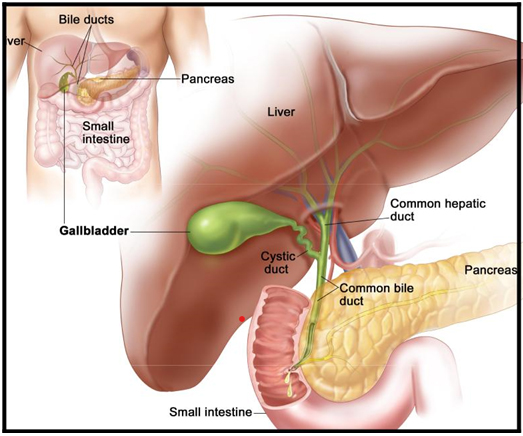
Gall bladder is located beneath the liver on the right side of the abdomen.The gall bladder stores bile, a digestive fluid produced by your liver. If diagnosed early, they have good very good survival rates.
Gall bladder cancer is fairly common in India, especially in the Northern parts.
It usually presents in 6th or 7th decade of life and is 2-3 times more common in women.
Risk factors for gall bladder cancer :
- Female gender / old age
- Gall stomnes, polyps >1 cms
- Parasitic infections
- Choledochal cyst
- Abnormal pancreatico-biliary duct junction
Symptoms and signs:
- Abdominal pain, particularly in the upper right portion of the abdomen
- Abdominal bloating
- Fever
- Significant loss of weight
- Nausea
- Yellowing of the skin and whites of the eyes (jaundice)
- Generalised itching all over body.
Diagnosis of gall bladder cancer:
Physical examination: Your doctor will examine your abdomen to look for any lump in the upper abdomen on the right side. Your eyes and skin will be examined to look for signs of jaundice
Blood investigations: Complete blood count, Liver function test, Viral markers , coagulation profile, CA19-9, CEA, Serum electrolytes, RFT
Radiological imaging: USG Abdomen, Triple phase CT scan of the abdomen, MRCP (if the tumour is invading the bile ducts), PET-CT scan
Biopsy: USG/CT guided biopsy when patient is planned for Neoadjuvant treatment (chemo or radiation ). If disease is operable , biopsy is not required.
If the patient presents with signs & symptoms of obstructive jaundice patient will be advised to get a ERCP or PTBD done to relieve the symptoms of obstructive jaundice and will allow the liver to recover from jaundice. Patients who will be candidate for surgical resection this will be done prior to surgery.Patients who are candidate for surgical resection will have a diagnostic laparoscopy at the time of surgery to assess the operability.
Treatment options for gall bladder cancer:
Surgery : Surgery for the gall bladder cancer depends on the stage of the
If the disease is confined to Gall bladder, then patient will require Radical
cholecystectomy with wedge resection of the liver(4b/5 segments) with portal lymphadenectomy with or without bile duct resection based on the extent of disease (Cystic duct margin will be sent for Frozen Section and if positive then bile duct resection will be performed). If there is a major infiltration into the liver or there is involvement of vessels supplying right lobe of liver , then the patient might require a major hepatectomy.
Some patients will get diagnosed of gall bladder cancer after undergoing laparoscopic cholecystectomy for the gall stones, this is defined as incidental gall bladder cancer. These patients will require a triple phase CT/ PET scan to look for residual disease. And based on histopathology report and imaging findings, they may need to undergo revision surgery after 4-6 weeks from the initial surgery.A Diagnostic Laproscopy will be performed in such cases to assess operability at the time of surgery.
We are one of the few centres in the country who offer major and aggressive surgical resections for gall bladder cancer with a good success rate and outcomes.
Chemotherapy and radiotherapy: This is considered in patients with potentially unresectable gall bladder cancer or gall bladder cancer with widespread metastasis or technically resectable gall bladder cancer but patient is not a candidate for major surgical resection
Palliative care: Palliative care is given to patients who are not a candidate for surgical resection. Gall bladder cancer patients with obstructive jaundice will be advised to undergo ERCP or PTBD to relieve them of obstructive jaundice symptoms. Usually a metal stent is placed in such cases to relieve the jaundice.
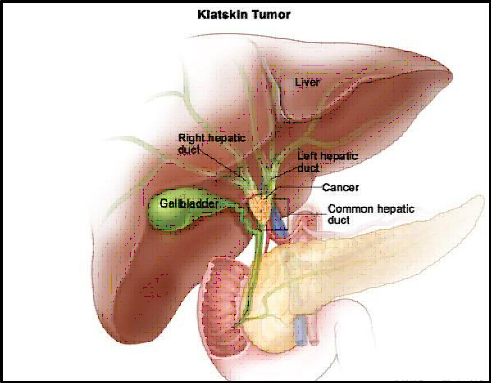
Hilar Cholangiocarcinoma:
Hilar cholangiocarcinoma (Klatskin’s tumour) is the cancer involving the confluence of right and left hepatic ducts.
The majority of patients are greater than 65 years of age. Cholangiocarcinoma may arise anywhere within the biliary tree but tumors involving the biliary confluence (hilar cholangiocarcinoma) are the most common.
Signs and symptoms
- Jaundice (yellowish discolouration of eyes and skin)
- Pain abdomen
- Loss of weight and appetite
- Fever with chills and rigor in case of cholangitis
- Fatigue
Risk factors for hilar cholangiocarcinoma
- Primary sclerosing cholangitis
- Age more than 50 yrs
- Parasitic infection( clonorchis sinensis & opisthorchisviverreni)
- Chronic liver disease
- Smoking
- Choledochal cysts
- Congenital hepatic fibrosis
- Hepatitis B and Hepatitis C infection
- Obesity and diabetes
- Chemical compounds(dioxin, thorotrast)
Treatment options for hilar cholangiocarcinoma
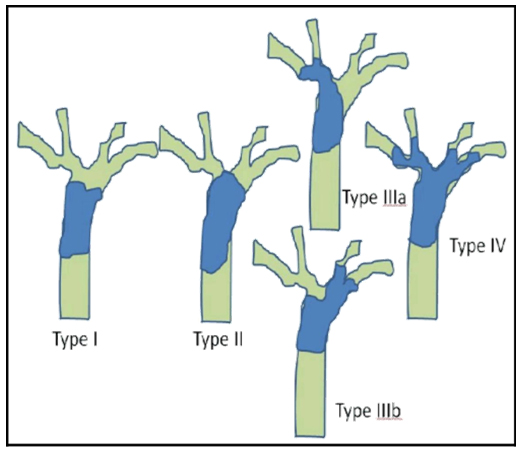
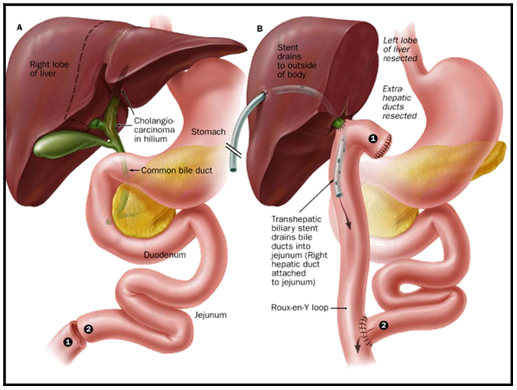
- Surgery: Major hepatectomy combined with extra hepatic bile duct resection has increased the long term survival and should be considered standard therapy. Bismuth Collarette classification helps to classify the disease and accordingly surgery is done. Usually, Bismuth-Corlette type I patients undergo Radical bile duct excision with hepaticojejunostomy. Type II & III lesions require Major Hepatectomy ( Right/ Left ) with hepaticojejunostomy.
- Chemotherapy and Radiotherapy: chemotherapy and radiotherapy is considered for locally advanced and unresectable hilar cholangiocarcinoma.It can be given in the neoadjuvant setting to downsize the tumour and based on the response of the tumour, they can be taken up for the surgery.
- Palliative care: If the patient is having a unresectable hilar cholangiocarcinoma or if the patient is not a candidate for major surgical resection then palliative care in the form of ERCP or PTBD is done to relieve the patients of obstructive jaundice symptoms.
-
Do gallstones cause gallbladder cancer?
-
what is do I expect after a surgery for gall bladder cancer?Patients who undergo radical cholecystectomy with wedge resection of liver will have a hospital stay of 4-5 days after surgery. They will be started on orals feeds after 48 hrs. If the patient requires a more aggressive surgery in the form of major hepatectomy then the hospital stay could be extended by few days depending on the recovery
-
Will I require chemotherapy or radiotherapy after surgery?Patients with advanced gall bladder cancer or hilar cholangiocarcinoma will require multi disciplinary treatment modalities.
-
What are the side effects of of chemotherapy and radiotherapy?Radiation therapy may cause patients to become very tired as treatment continues. In addition, when patients receive radiation therapy, the skin in the treated area may sometimes become red, dry, and tender. Radiation therapy to the abdomen may cause nausea, vomiting, diarrhea, or other problems with digestion. For most patients, the side effects of radiation therapy go away when treatment is over.Patients who undergo chemotherapy may also be more likely to get infections, bruise or bleed easily, and may have less energy. Other side effects such as poor appetite, nausea and vomiting, diarrhea, or mouth sores. Usually, these side effects go away gradually during the recovery periods between treatments or after treatment is over.
-
What is the survival rate in hilar cholangiocarcinoma?Survival depends on the stage of the cancer at the time of diagnosis. Most of the patients get diagnosed in advanced stages.5 year survival in node negative disease its 50%. In node positive disease its 35% In inoperable cases prognosis is very poor with 5 year survival rate of less than 5%
-
What are the complications of surgery for gall bladder and bile duct cancers?Bile leak, abdominal collections, wound infection, pneumonia. All these complications are managed conservatively. Rare complications include intra abdominal haemorrhage which may require surgery.
-
What is the follow up period after surgery?In the first year its every 3 months. After 1 year its every 6 months
-
What is the survival rate in gall bladder cancer?5 year survival rate for resectable node negative disease is around 40% and node positive disease is 25%. Inoperable cases have extremely poor prognosis.